Frozen Shoulder vs Arthritis: Differences
Learn how to tell frozen shoulder apart from arthritis. Compare symptoms, causes, and treatments to get the right diagnosis.
By Joint Pain Authority Team
Quick Answer
Frozen shoulder (adhesive capsulitis) and shoulder arthritis both cause pain and stiffness, but they are fundamentally different conditions. Frozen shoulder involves the joint capsule tightening and restricting movement in all directions, even when someone else moves your arm. Arthritis involves cartilage wearing away from the bone surfaces. Frozen shoulder typically resolves in 1-3 years. Arthritis is progressive and permanent. Treatment plans differ significantly, making accurate diagnosis essential.
The Core Difference
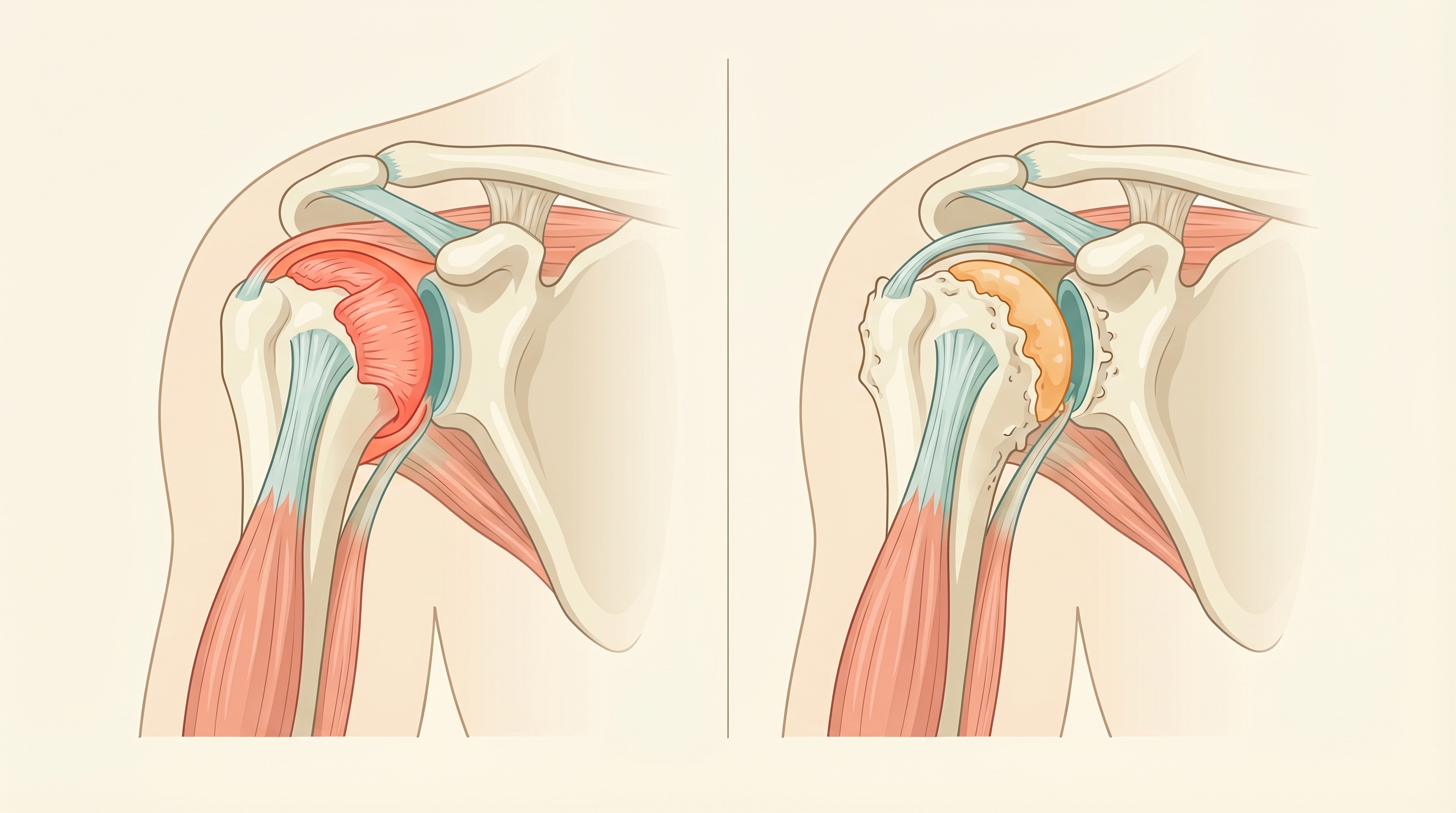
Frozen shoulder is a capsule problem. The tissue surrounding your shoulder joint thickens and tightens, forming adhesions that restrict movement. The joint surfaces themselves are healthy.
Shoulder arthritis is a cartilage problem. The smooth surfaces inside the joint wear down, causing bone-on-bone contact. The joint capsule may stiffen secondarily, but the root cause is surface damage.
Think of it this way: frozen shoulder is like a door with rusted hinges that will not open. Arthritis is like a door where the hinge pin is worn down to nothing.
How Symptoms Compare
Pain Patterns
| Feature | Frozen Shoulder | Shoulder Arthritis |
|---|---|---|
| Pain location | Outer shoulder and upper arm | Deep inside the joint |
| Pain quality | Sharp with sudden movements | Dull, aching, grinding |
| Night pain | Severe, often the worst symptom | Common but varies |
| Pain trigger | Reaching beyond restricted range | All shoulder movements |
| Pain progression | Increases then plateaus, then improves | Gradually worsens over time |
Movement Restrictions
This is the most reliable way to tell the two conditions apart.
Frozen shoulder restricts passive movement. When your doctor or therapist tries to move your arm for you (while you relax completely), the arm will not move past certain points. This happens because the capsule itself is physically shortened and tight.
Arthritis restricts active movement more than passive. Your arm may go further when someone else moves it for you because the issue is pain and grinding, not a physical barrier. Passive motion is reduced but not as dramatically “stuck” as frozen shoulder.
Progression Timeline
Frozen Shoulder Stages
- Freezing (2-9 months): Pain increases gradually, motion decreases
- Frozen (4-12 months): Pain may lessen, but stiffness is at its worst
- Thawing (5-24 months): Motion gradually returns
- Resolution: Most regain full or near-full motion
Total duration: 1-3 years (self-limiting)
Arthritis Progression
- Early: Occasional aching, mild stiffness
- Moderate: Regular pain, noticeable motion loss, crepitus
- Severe: Constant pain, significant disability
- End-stage: Bone-on-bone, may need replacement
Total duration: Progressive and permanent without treatment
Who Gets Each Condition?
Frozen Shoulder Risk Factors
- Age 40-60 (most common onset)
- Women more than men (70% of cases)
- Diabetes (10-20% of diabetics develop frozen shoulder)
- Thyroid disorders
- Recent immobilization (after surgery, fracture, or stroke)
- Parkinson’s disease
- Heart disease
Arthritis Risk Factors
- Age over 50-60 (incidence increases with age)
- Men and women equally after age 60
- Previous shoulder injury (fracture, dislocation)
- Repetitive overhead work or sports
- Rotator cuff damage (alters joint mechanics)
- Family history of arthritis
- Obesity (systemic inflammation)
Yes. Some patients develop adhesive capsulitis on top of existing arthritis, especially after a period of reduced movement due to arthritis pain. This combination requires careful diagnosis because the treatment approach must address both issues.
How Doctors Tell Them Apart
Physical Examination Clues
Your doctor will test both active range of motion (you move your arm) and passive range of motion (they move your arm while you relax).
Frozen shoulder hallmarks:
- Equal loss of active and passive motion
- External rotation is often the most restricted direction
- Movement hits a firm endpoint, like hitting a wall
- Crepitus (grinding) is absent
Arthritis hallmarks:
- Passive motion is somewhat better than active
- Grinding or crunching sensation during movement
- Tenderness directly over the joint
- Motion loss is gradual and in all directions
Imaging Differences
X-rays:
- Frozen shoulder: X-rays look normal. No bone spurs, no joint space narrowing
- Arthritis: Visible joint space narrowing, bone spurs, surface irregularity
MRI:
- Frozen shoulder: Thickened joint capsule, sometimes visible adhesions
- Arthritis: Cartilage thinning, bone marrow changes, possible rotator cuff damage
The X-ray is often the deciding test. If the joint surfaces look healthy, frozen shoulder is more likely. If there is visible cartilage loss and bone changes, arthritis is the diagnosis.
Treatment: Different Approaches
Treating Frozen Shoulder
The goal is to restore motion while managing pain. Because frozen shoulder is self-limiting, treatment focuses on speeding recovery and reducing suffering during the process.
Physical therapy is the cornerstone. Gentle stretching within pain tolerance gradually restores range of motion. Aggressive stretching can worsen inflammation and slow recovery.
Cortisone injections reduce inflammation inside the capsule and can significantly improve pain and motion, especially in the freezing and frozen stages.
Hydrodilatation is a procedure where fluid is injected into the joint capsule under pressure to stretch it open. Some studies show it speeds recovery.
Manipulation under anesthesia involves putting you to sleep and manually breaking up the adhesions. Reserved for cases that do not respond to other treatments.
Surgery (arthroscopic capsular release) cuts through the thickened capsule to restore motion. Rarely needed.
Treating Shoulder Arthritis
The goal is to manage pain, maintain function, and slow progression. Because arthritis is permanent, treatment is ongoing.
Physical therapy focuses on strengthening the rotator cuff, maintaining range of motion, and correcting movement patterns.
Medications include NSAIDs, topical treatments, and acetaminophen for pain control.
Cortisone injections provide temporary anti-inflammatory relief (4-12 weeks).
Hyaluronic acid (gel) injections lubricate and cushion the joint, providing longer-lasting relief (3-6 months). Evidence for shoulder use is growing.
Shoulder replacement surgery is considered for severe, end-stage arthritis that does not respond to other treatments.
Read: Shoulder Osteoarthritis Complete Guide
Shoulder Pain Answers in Your Inbox
Get evidence-based guides on diagnosis, treatment options, and daily management for shoulder conditions.
Join 10,000+ readers. No spam.
Key Takeaway: Why Diagnosis Matters
Getting the right diagnosis changes everything about your treatment plan.
If you treat frozen shoulder like arthritis, you may pursue injections or surgical consultations you do not need. Frozen shoulder resolves on its own. The right approach is stretching, pain management, and patience.
If you treat arthritis like frozen shoulder, you may wait for improvement that never comes. Arthritis requires an active, stepwise treatment plan because it does not resolve on its own.
Both conditions cause real pain and frustration. But knowing which one you have puts you on the right path.
Frequently Asked Questions
How can I tell at home if I have frozen shoulder or arthritis?
Try this simple test: stand with your arm at your side, elbow bent to 90 degrees, and rotate your forearm outward (like opening a door). If that motion is severely restricted and hits a hard stop, frozen shoulder is more likely. If the motion is painful and grinding but goes further, arthritis is more common. However, you need imaging to confirm either diagnosis.
Does frozen shoulder always go away on its own?
Most cases resolve within 1-3 years, though some patients retain mild motion loss permanently. Treatment can speed recovery and reduce pain during the process. Diabetic patients tend to have longer courses and more residual stiffness.
Can gel injections help frozen shoulder?
Hyaluronic acid injections are designed for arthritis (cartilage loss), not frozen shoulder (capsule tightness). Cortisone injections are more appropriate for frozen shoulder because they reduce the inflammation driving the capsule tightening.
I have diabetes and shoulder stiffness. Which condition is more likely?
Diabetes significantly increases frozen shoulder risk. Up to 20% of diabetics develop adhesive capsulitis. However, diabetes also increases arthritis risk through inflammatory pathways. Your doctor can distinguish them with an X-ray.
Can frozen shoulder come back after it resolves?
Recurrence in the same shoulder is uncommon (about 5-10%). However, frozen shoulder in the opposite shoulder occurs in 20-30% of cases, often within 5 years of the first episode.
Should I push through the pain to stretch a stiff shoulder?
If you have frozen shoulder, gentle stretching within tolerance is helpful. Aggressive forcing can worsen inflammation. If you have arthritis, stretching is important but should focus on maintaining motion, not pushing through sharp pain. A physical therapist can guide the right intensity for either condition.
Related Resources
Enjoyed this article?
Get more insights like this delivered to your inbox weekly.
Join 10,000+ readers. No spam.