Genicular Artery Embolization (GAE): Complete Guide
Genicular artery embolization (GAE) is a minimally invasive outpatient procedure that blocks abnormal blood vessels feeding knee inflammation. Learn how it works, who qualifies, recovery, and costs.
By Joint Pain Authority Team
Quick Answer
Genicular artery embolization (GAE) is a minimally invasive, outpatient procedure where an interventional radiologist blocks tiny abnormal blood vessels that feed inflammation in the knee. Studies show 92% of patients met the WOMAC pain improvement threshold at 12 months, and only 5.2% needed a knee replacement within two years. The procedure takes about one hour under local anesthesia, and most patients walk the same day.
What Is Genicular Artery Embolization?
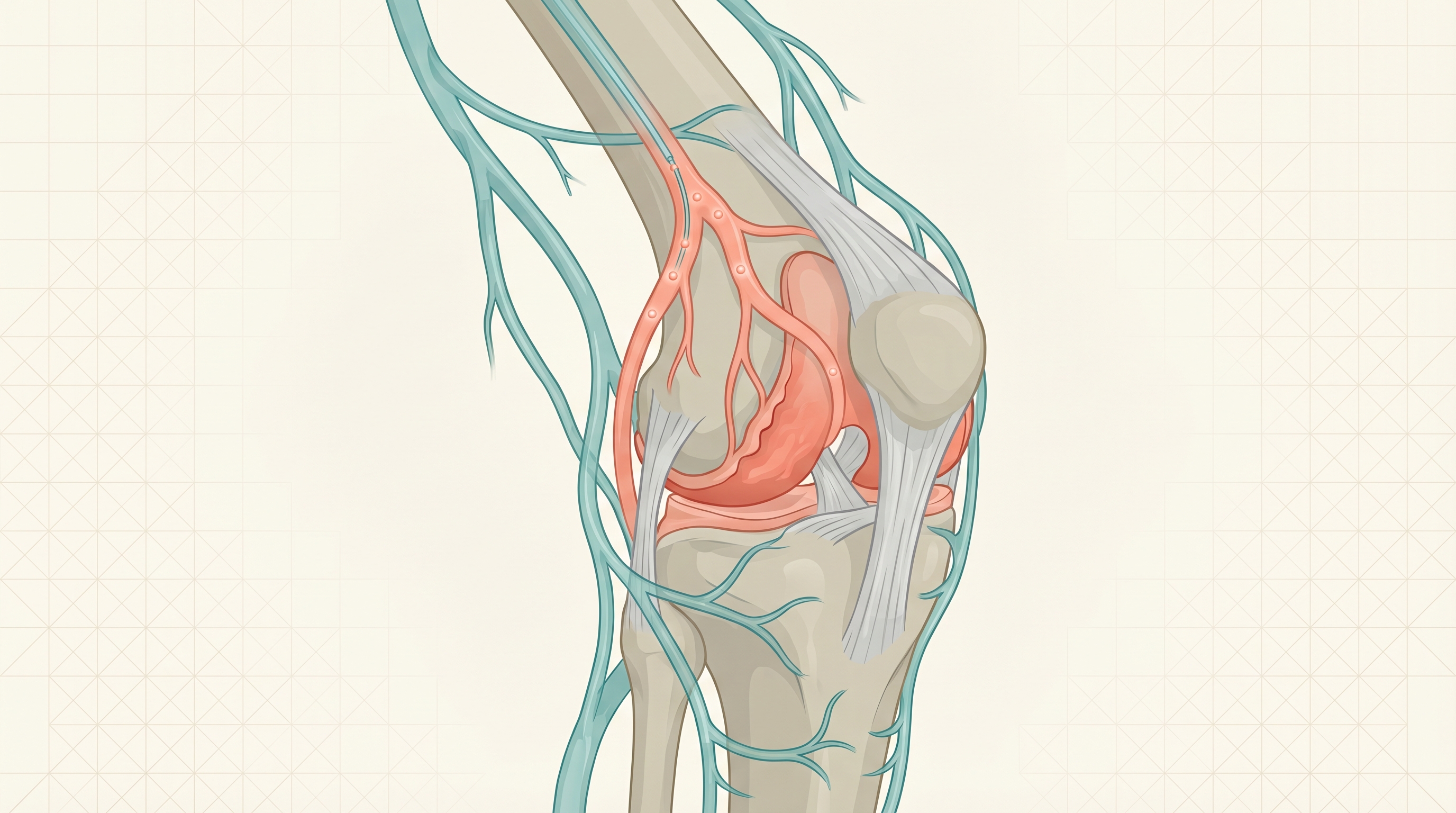
GAE is a catheter-based procedure that targets the root cause of inflammatory knee pain: abnormal new blood vessels (called neovascularity) that grow into the lining of arthritic joints. These vessels bring nerve fibers and inflammatory cells that amplify pain far beyond what the structural damage alone would cause.
During GAE, an interventional radiologist threads a tiny catheter through a pinhole incision in the wrist or groin, guides it to the knee’s genicular arteries using live X-ray imaging, and injects microscopic beads (microspheres) that block the abnormal vessels. The procedure essentially cuts off the blood supply that feeds knee inflammation.
How GAE Differs From Other Treatments
| Factor | GAE | Cortisone Injections | Gel Injections | Knee Replacement |
|---|---|---|---|---|
| Approach | Blocks abnormal blood vessels | Reduces inflammation chemically | Restores joint lubrication | Replaces the joint |
| Anesthesia | Local (awake) | None/local | None/local | General/spinal |
| Procedure time | ~1 hour | 5-10 minutes | 5-10 minutes | 1-2 hours |
| Recovery | 1-2 days | 24-48 hours | 24-48 hours | 3-6 months |
| Duration of relief | 12+ months (early data) | Weeks to months | 6-12 months | 15-20 years |
| Repeatable | Yes | Limited (3-4x/year) | Yes | Revision only |
How the Procedure Works
Before the Procedure
During the Procedure (~1 Hour)
- Local anesthesia numbs the catheter entry site (usually wrist or upper thigh)
- A micro-catheter (about the width of a spaghetti strand) is guided to the genicular arteries
- Contrast dye identifies the abnormal blood vessels on live imaging
- Tiny microspheres (smaller than a grain of sand) are injected to block those vessels
- The radiologist confirms the abnormal vessels are blocked
- The catheter is removed and a small bandage is placed
After the Procedure
- Most patients walk out of the facility the same day
- Mild soreness or bruising at the catheter site for a few days
- Some patients notice improvement within days; for others it takes 1-3 months
- Follow-up appointment typically at 1 month and 3 months
Who Is a Good Candidate for GAE?
Ideal Candidates
May Not Be Ideal For
What Does the Evidence Say?
GAE is a newer procedure, but early results from clinical trials are encouraging.
Key Study Results
| Study | Finding |
|---|---|
| GENESIS Trial | Landmark U.S. randomized controlled trial demonstrating significant pain reduction vs. sham procedure |
| 12-Month Outcomes | 92% of patients met the WOMAC Minimum Clinically Important Difference (MCID) for pain improvement |
| Surgery Avoidance | Only 5.2% of GAE patients went on to need total knee replacement within 2 years |
| Multi-Center Data | Consistent positive results from studies in Japan, Europe, and the United States |
What WOMAC MCID Means
The WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) is the gold standard for measuring osteoarthritis outcomes. The MCID is the smallest improvement that patients consider meaningful. When 92% of patients meet this threshold, it means the vast majority experienced real, noticeable relief.
Risks and Side Effects
Like any medical procedure, GAE carries some risks, though serious complications are uncommon.
Common (usually mild and temporary):
- Bruising at the catheter entry site
- Minor skin discoloration near the knee (resolves in weeks)
- Temporary increase in knee discomfort for a few days
Rare:
- Skin ulceration near the knee (reported in early studies using larger particles; newer techniques have reduced this risk)
- Non-target embolization (blocking vessels not intended; experienced operators minimize this)
- Allergic reaction to contrast dye
The overall safety profile in published studies has been favorable. Most side effects are mild and self-limiting. Using smaller microspheres and advanced imaging has improved safety compared to early procedures.
Current Availability
GAE is not yet widely available. It is performed at specialized interventional radiology centers, typically at academic medical centers or larger hospital systems. Availability is growing as more interventional radiologists are trained in the technique and as clinical trial data continues to build.
To find a provider, ask your doctor for a referral to an interventional radiologist who performs GAE, or contact the interventional radiology department at a major medical center near you.
Get Emerging Treatment Updates
Be the first to know about new minimally invasive options for knee pain, including GAE developments and clinical trial results.
Join 10,000+ readers. No spam.
Frequently Asked Questions
Is GAE FDA-approved?
GAE uses FDA-cleared devices (catheters and microspheres) that are already approved for other embolization procedures. The application to knee osteoarthritis is considered an off-label but evidence-supported use. Clinical trials like the GENESIS trial are building the evidence base for wider adoption.
How much does GAE cost?
Out-of-pocket costs typically range from $5,000 to $15,000 depending on the facility and your insurance coverage. Some Medicare and private insurance plans have begun covering GAE using existing interventional radiology billing codes, but coverage is not yet universal. See our GAE cost and insurance guide for a detailed breakdown.
How long do the results last?
Published studies show significant pain relief lasting at least 12 months. Longer-term data (2-3 years) from ongoing studies is encouraging, with the 5.2% knee replacement rate at two years suggesting durable benefit. Since this is a newer procedure, 5- and 10-year data is not yet available.
Can GAE be repeated if needed?
Yes. If symptoms return after initial improvement, GAE can be repeated. Some patients may develop new abnormal vessels over time that can be treated with a second procedure.
Does GAE replace gel injections or cortisone?
Not necessarily. GAE targets a different mechanism (abnormal blood vessel growth) than gel injections (lubrication) or cortisone (chemical inflammation). Some patients may benefit from combining GAE with other treatments. Many GAE candidates are patients who have already tried and had limited success with cortisone or gel injections.
How do I know if GAE is right for me?
Start by discussing it with your orthopedist or primary care doctor. If you have moderate knee osteoarthritis with an inflammatory component and have not gotten adequate relief from conservative treatments, ask for a referral to an interventional radiologist who performs GAE.
This article is for informational purposes only and does not replace medical advice. Consult with your healthcare provider about whether GAE is appropriate for your individual situation.
Last reviewed: April 2026
Related Resources
Enjoyed this article?
Get more insights like this delivered to your inbox weekly.
Join 10,000+ readers. No spam.