Gout in the Knee: Symptoms, Causes & Treatment
Gout in the knee causes sudden, intense pain and swelling. Learn how knee gout differs from other joints, how it's diagnosed, and the best treatments for fast relief.
By Joint Pain Authority Team
Quick Answer
Gout in the knee causes sudden, severe pain, redness, warmth, and swelling that often strikes at night. Unlike knee osteoarthritis, which develops slowly over months, a knee gout attack reaches peak intensity within 12 to 24 hours. Diagnosis requires a joint fluid test showing uric acid crystals, and treatment combines anti-inflammatory medications with long-term uric acid control.
Why Gout Targets the Knee
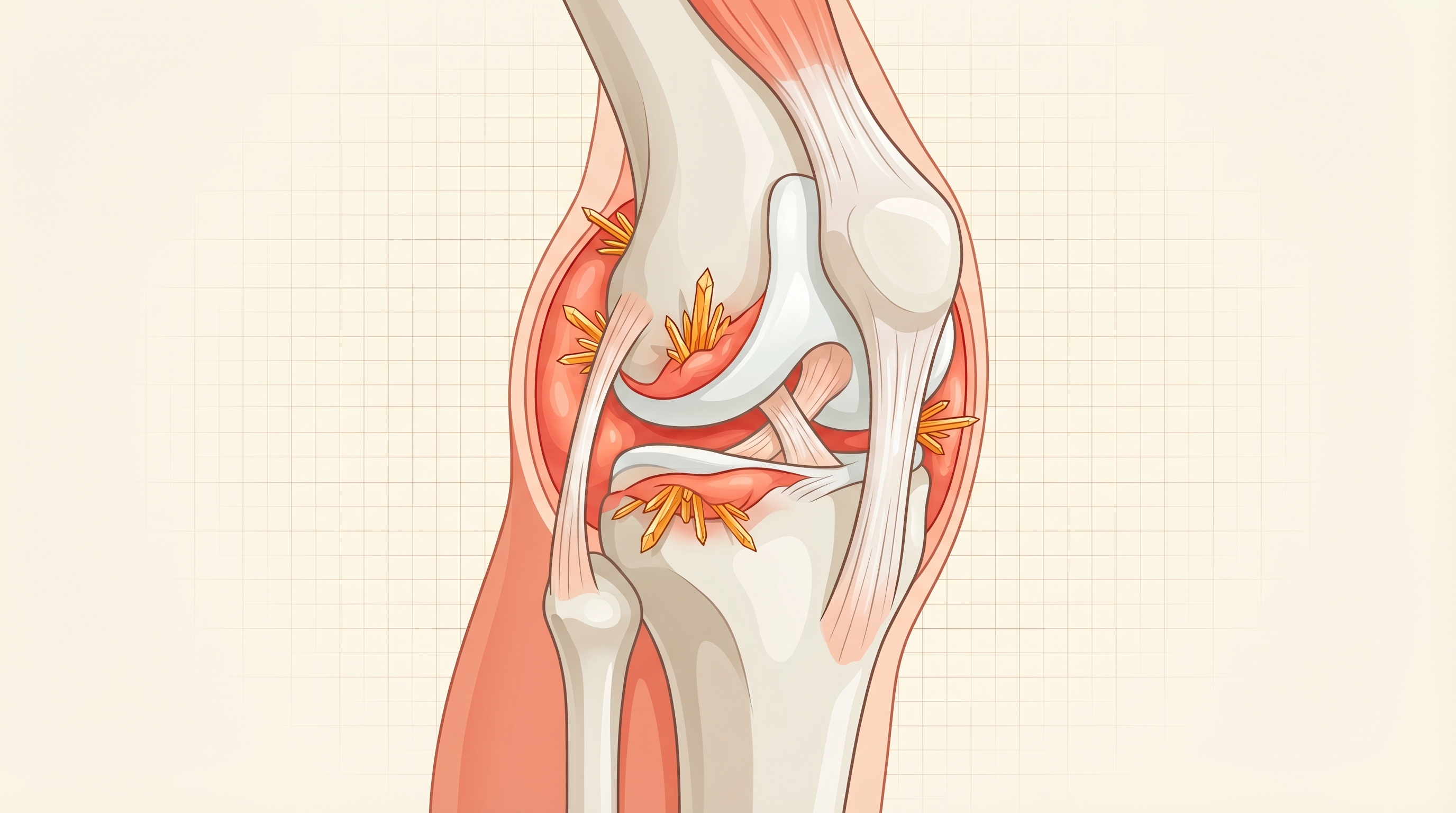
Gout is caused by a buildup of uric acid in the blood (hyperuricemia). When levels get too high, uric acid forms sharp, needle-like crystals that deposit in joints. While the big toe is the most famous gout target, the knee is the second most commonly affected large joint, involved in roughly 25-30% of gout cases according to data published in Arthritis Care & Research.
The knee is particularly vulnerable because:
- Lower body temperature — Uric acid crystals form more easily at cooler temperatures. The knee’s large surface area loses heat readily.
- Weight-bearing stress — Mechanical stress on the joint can trigger crystal shedding from cartilage surfaces.
- Existing damage — If you already have knee osteoarthritis, damaged cartilage provides more surfaces for crystal deposition. A 2023 study in Annals of the Rheumatic Diseases found that 18% of patients with knee OA also had uric acid crystals in their synovial fluid.
Knee Gout Symptoms vs. Other Joints
Gout in the knee shares the hallmark features of gout anywhere — sudden onset, severe pain, and inflammation — but there are important differences compared to gout in smaller joints like the big toe.
| Feature | Knee Gout | Big Toe Gout |
|---|---|---|
| Pain severity | Severe, deep ache | Excruciating surface pain |
| Swelling | Large visible effusion (fluid) | Localized swelling |
| Mobility impact | Cannot bend or bear weight | Cannot wear shoes, walk |
| Warmth/redness | May be subtle over large area | Obvious bright red skin |
| Mistaken for | Septic joint, OA flare, pseudogout | Bunion, fracture, cellulitis |
| Duration | 7-14 days untreated | 5-10 days untreated |
The Telltale Signs of Knee Gout
Sudden onset — You go to bed feeling fine and wake up at 2 AM with a swollen, hot knee. This “overnight attack” pattern is a classic gout signature. It happens because body temperature drops during sleep, and cortisol (which suppresses inflammation) reaches its lowest level at night.
Extreme tenderness — Even the weight of a bedsheet on your knee can be agonizing. The medical term is “exquisite tenderness,” and it’s far more intense than a typical osteoarthritis flare.
Visible swelling — A gout-affected knee can swell dramatically within hours. The joint may produce so much fluid that it appears balloon-like compared to the other knee.
Skin changes — The skin over and around the knee may turn red or purplish and feel warm to the touch. As the attack resolves over days, the skin sometimes peels.
Fever and chills — Unlike OA flares, a severe knee gout attack can cause systemic symptoms including low-grade fever (up to 101 degrees F), chills, and general malaise. This overlap with joint infection is why getting a proper diagnosis matters urgently.
How Knee Gout Is Diagnosed
Because a hot, swollen knee can signal a dangerous joint infection, doctors take knee gout seriously and typically perform several tests.
Joint Aspiration (Arthrocentesis)
This is the gold standard. A doctor uses a needle to withdraw fluid from the swollen knee. Under a polarized microscope, uric acid crystals appear as needle-shaped, negatively birefringent crystals — a finding that is 100% specific for gout. This test also rules out infection (septic arthritis), which requires emergency treatment.
Blood Tests
- Serum uric acid — Levels above 6.8 mg/dL are considered elevated. However, uric acid can be normal during an acute attack in up to 40% of patients, so a normal result does not rule out gout.
- Inflammatory markers — ESR and CRP are typically elevated during a flare.
- Complete blood count — White blood cells may be elevated, mimicking infection.
Imaging
- X-rays — May show soft tissue swelling during acute attacks. In chronic gout, X-rays can reveal characteristic “punched-out” bone erosions with overhanging edges.
- Dual-energy CT (DECT) — Can detect uric acid crystal deposits in joints with 90% sensitivity. Increasingly used when joint aspiration is difficult or when chronic gout is suspected.
- Ultrasound — Can show the “double contour sign” — a bright line on the cartilage surface caused by crystal deposits — with 80% specificity for gout.
Treating an Acute Knee Gout Attack
The goal during an attack is rapid pain relief and inflammation control. Treatment works best when started within the first 24 hours.
First-Line Medications
Colchicine — Most effective when taken within 12 hours of symptom onset. The standard dose is 1.2 mg followed by 0.6 mg one hour later. A landmark trial in the New England Journal of Medicine showed this low-dose regimen was as effective as high-dose colchicine but with 75% fewer side effects.
NSAIDs — Indomethacin (50 mg three times daily) or naproxen (500 mg twice daily) for 5-7 days. These work well but should be used cautiously in patients over 65 due to kidney and stomach risks.
Corticosteroids — For patients who cannot take colchicine or NSAIDs, oral prednisone (30-40 mg daily, tapered over 7-10 days) or a corticosteroid injection directly into the knee provides rapid relief. Joint injection has the advantage of targeted treatment with fewer systemic side effects.
Home Management
- Ice the knee — Apply ice packs for 20 minutes at a time, several times daily. A 2021 study found that ice application during gout attacks reduced pain scores by 2 points on a 10-point scale.
- Elevate the leg — Keep the knee above heart level to reduce swelling.
- Stay hydrated — Drink at least 8-10 glasses of water daily to help flush uric acid.
- Rest the joint — Avoid bearing weight during the acute phase.
Preventing Future Knee Gout Attacks
Once you have had one knee gout attack, there is approximately a 60% chance of a second attack within one year without preventive treatment, according to the American College of Rheumatology.
Uric Acid-Lowering Therapy
Your doctor may recommend long-term medication if you have 2 or more attacks per year, tophi (uric acid lumps), or kidney stones. The target is a serum uric acid level below 6.0 mg/dL.
- Allopurinol — The most commonly prescribed uric acid-lowering drug. Starting dose is typically 100 mg daily, gradually increased. Effective and affordable.
- Febuxostat (Uloric) — An alternative when allopurinol is not tolerated. A 2018 trial showed slightly higher cardiovascular risk, so it is used as a second-line option.
For a comprehensive look at all gout medications and newer treatments, read our guide on gout treatment options.
Diet and Lifestyle Changes
Diet accounts for about 12% of uric acid variation, but targeted changes can meaningfully reduce flare risk:
- Limit red meat, organ meats, and shellfish
- Avoid beer and limit liquor
- Eat more low-fat dairy, cherries, and vitamin C-rich foods
- Stay well hydrated
See our complete gout diet plan for detailed food lists and meal ideas.
Get weekly joint pain relief tips
Evidence-based strategies for managing gout, arthritis, and joint pain delivered to your inbox.
Join 10,000+ readers. No spam.
When Knee Gout and Knee OA Overlap
Having both gout and osteoarthritis in the same knee is more common than many people realize. Research in Arthritis & Rheumatology found that gout patients are 1.5 to 2 times more likely to develop knee OA, partly because repeated crystal-driven inflammation damages cartilage over time.
If you have both conditions:
- Knee pain between gout attacks may be OA, not “mild gout”
- Treatment must address both: uric acid control for gout, plus physical therapy and possibly hyaluronic acid injections for OA
- Weight management is doubly important — excess weight raises uric acid and increases knee joint stress
Frequently Asked Questions
Can gout affect both knees at the same time?
Yes, though it is less common than a single-knee attack. Bilateral (both knees) gout occurs in roughly 10-15% of knee gout episodes and is more likely in patients with very high uric acid levels or those who are not on preventive medication.
How can I tell if my knee pain is gout or osteoarthritis?
The speed of onset is the biggest clue. Gout attacks reach peak pain within 12-24 hours and the knee is hot, red, and markedly swollen. OA pain develops gradually, worsens with activity, and improves with rest. If you are unsure, a joint fluid aspiration can provide a definitive answer.
Is knee gout more common in men or women?
Gout overall is about 3-4 times more common in men. However, after menopause, women’s gout rates increase significantly because estrogen (which helps kidneys excrete uric acid) declines. In patients over 65, the gender gap narrows considerably.
How long does a knee gout attack last?
Without treatment, a knee gout attack typically lasts 7-14 days — longer than gout in smaller joints. With prompt treatment (started within 24 hours), most patients experience significant relief within 2-3 days. Learn more in our gout flare-up management guide.
Can knee gout cause permanent damage?
Yes, if not properly managed. Repeated gout attacks cause chronic inflammation that erodes cartilage and bone over time. A study in Rheumatology found that patients with more than 5 gout flares had measurable joint damage on imaging. This is why preventive treatment with uric acid-lowering therapy is essential.
Should I exercise during a knee gout flare?
No. Rest the knee completely during an acute attack. Exercise during a flare can worsen pain and prolong the episode. Once the flare resolves completely (usually 1-2 weeks), gentle exercise like walking or aquatic therapy can resume gradually.
The information in this article is for educational purposes only and is not intended as medical advice. Always consult with your healthcare provider for diagnosis and treatment of gout or any joint condition.
Last medically reviewed: April 2026
Enjoyed this article?
Get more insights like this delivered to your inbox weekly.
Join 10,000+ readers. No spam.